What It Actually Takes to Reform Healthcare in Western Uusimaa
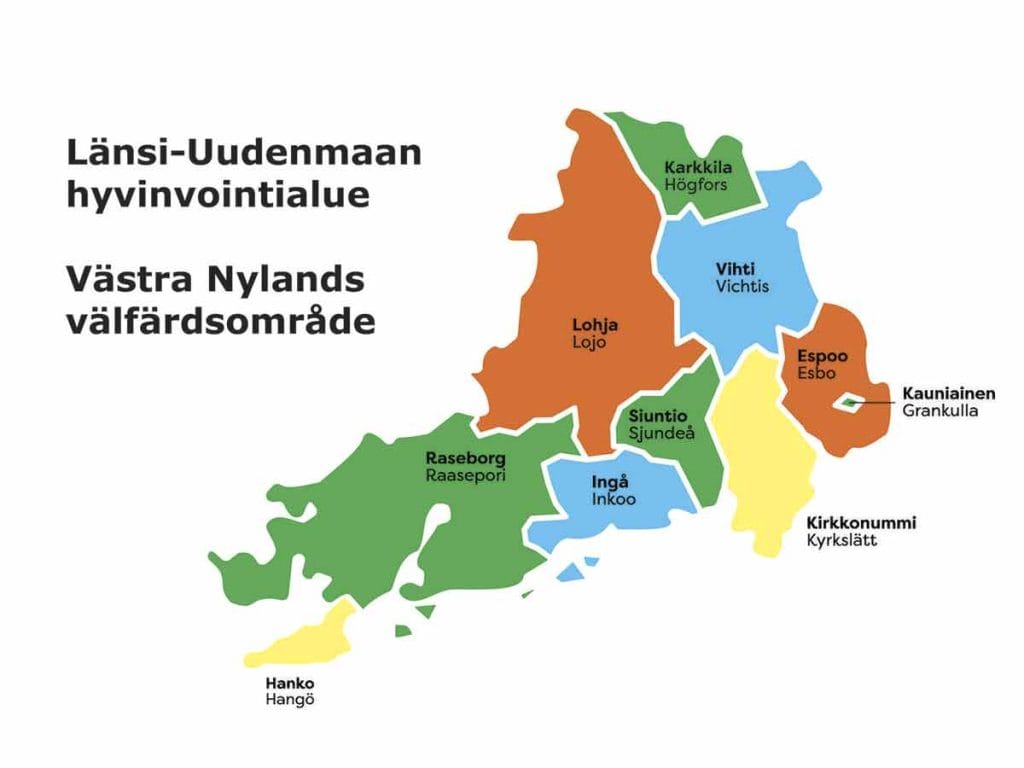
In January 2023, Finland did something that most countries only talk about. It consolidated its fragmented municipal health and social services into 21 regional wellbeing services counties, each responsible for delivering care to hundreds of thousands of residents. The idea was ambitious and the execution was chaotic. Ten distinct city administrations (Espoo, Kirkkonummi, Lohja, Raasepori, Hanko, Inkoo, Karkkila, Kauniainen, Siuntio, and Vihti), five municipal federations, a decade of legacy IT systems, and nearly 10,000 employees had to be brought under one roof in Western Uusimaa alone.
I sit on the Services and Personnel Committee for this county as a deputy member. I also work in healthcare and research human behaviour. So I follow what happens in these meeting rooms closely, not just as a committee member reading budget documents, but as someone who sees the downstream effects on actual patients and colleagues. What I want to do here is translate what is happening in our county into language that anyone can understand, because the official documents are in Finnish, the meeting minutes are dense, and the reality of this reform deserves a wider audience.
The boring part that made everything else possible
The first eighteen months of the new county's existence were, from the outside, completely invisible. No one writes headlines about payroll harmonisation or the merging of patient record systems across ten municipalities. But that administrative stabilisation period, roughly 2022 through mid-2024, was the non-negotiable foundation for everything that followed. You cannot redesign how care is delivered if half your staff are still figuring out which HR system they belong to and the other half are working with incompatible patient data.
The county had a legal obligation, spelled out clearly in its founding documents, to establish sufficient staffing structures to organise operations and exercise public authority across the entire region. That meant creating a single organisation out of parts that had never been designed to fit together. Different pay scales. Different protocols for referrals. Different approaches to procurement. All of it had to be reconciled before anyone could even begin talking about improving the actual experience of care.
By late 2024, that phase was largely complete. The county had demonstrated it could keep the lights on during the transition. And that earned it something more valuable than any budget line: the credibility to start making structural changes.
Rethinking where people live and how they are cared for
One of the most significant shifts in the county's service strategy is the move toward what is called "yhteisöllinen asuminen," or community living. The concept sits in the space between full independence and institutional care. Rather than placing an elderly person in a traditional 24/7 residential facility the moment they can no longer manage entirely on their own, community living offers supported housing with shared spaces, social connection, and access to care staff without the rigidity or cost of full institutionalisation.
The county's targets for 2030 are striking. For residents aged 75 and over, the goal is to bring community living coverage to 2% of the population, up from a baseline of just 0.3%. For disability services, the target is 30% community-based housing, up from 12%. These are not small adjustments. They represent a fundamental rethinking of how care infrastructure is distributed.
The logic is both humane and fiscal. Loneliness and social isolation among older adults are not just quality of life problems. They are clinical risk factors that drive hospitalisation, cognitive decline, and depression. Community living addresses those risks while costing substantially less per person than round-the-clock institutional care. In an ageing society where the ratio of working-age taxpayers to retirees is shrinking year on year, this kind of structural redesign is the only way to keep the system viable without gutting the quality of what it provides.
New community living facilities are already being developed, including in Inkoo (Lönneberg) and Espoo (the Kauklahti live-and-reside senior centre), with additional capacity being procured from private providers [LUVN Budget 2025-2027].
Digital services as a survival strategy
There is a tendency to talk about digitalisation in healthcare as a modernisation project, a nice upgrade that makes things a bit more convenient. In Western Uusimaa, the digital service platform is nothing of the sort. It is a survival mechanism.
Here is the context. The county's specialised care is delivered through HUS, the Helsinki University Hospital federation. HUS is an enormous cost centre, and the pressure it puts on county budgets is constant. In late 2024, HUS sought a significant funding increase that, if absorbed in full, would have required broad cuts to local primary care services across the county.
This tension is not a one-off budget dispute. It is a structural feature of the SOTE reform itself. Counties are responsible for funding specialised hospital care delivered by HUS, but they have limited control over the volume or cost of that care. HUS sets its own service levels, its own staffing, its own investment priorities. The counties pay the bill. When HUS costs rise, the money has to come from somewhere, and that somewhere is almost always primary care, prevention, and social services, precisely the areas that reduce the need for hospital care in the first place. It is a system designed to cannibalise its own foundations.
The county's response was to accelerate its investment in primary care capacity, and digital tools are central to that.
The county's "spearhead projects" for 2025 include the procurement of a unified digital service platform and the rollout of synchronised client and patient information systems. Starting in 2025, residents gained access to digital messaging services for health centres, maternity clinics, and social services [LUVN Budget 2025-2027; LUVN Press Release, October 2024]. The county has also begun deploying AI-assisted tools for patient documentation and expanding a practitioner model ("ammatinharjoittajamalli") to improve continuity of care at health centres.
The strategic purpose is clear: if you can treat more people effectively at the primary care level, through digital access, faster triage, better documentation, and stronger local clinics, you reduce the flow of patients into expensive specialised hospital care. Every patient who gets adequate help from their local health centre is a patient who does not end up in an HUS emergency department at several times the cost.
The motivation is entirely defensive, born from the reality that the county's budget cannot absorb unchecked cost growth from specialised care without sacrificing the very primary services that prevent hospitalisations in the first place.
The fiscal tightrope, and how the county walked it
The financial constraints facing Western Uusimaa have been severe even by Finnish standards. Under the wellbeing services county legislation, accumulated deficits from 2023 and 2024 had to be covered by the end of 2026. Unlike many other counties in the Uusimaa region that were expected to miss this target, Western Uusimaa (along with Helsinki) was held to a strict legal ultimatum with no extensions.
The county's budget for 2025 contained no provision for new borrowing. Every investment had to be funded from carry-overs from previous years. The 2025 budget aimed for an 80 million euro surplus to make a serious dent in the accumulated deficit, while simultaneously pursuing a 30 million euro permanent reduction in the cost base [LUVN Budget 2025-2027; LUVN Press Release, October 2024].
The county's 2025 fiscal year ended with a surplus of 127.9 million euros, making Western Uusimaa the first wellbeing services county in Finland to fully cover its accumulated deficits [Länsiväylä, April 2026; Länsi-Uusimaa, April 2026]. But the headline number requires context. Of that surplus, 105.7 million euros came from a retroactive adjustment in state funding, a one-off correction that will not recur. Strip that away and the operational surplus was roughly 22 million euros. Still positive. Still ahead of nearly every other county in the country. But far less exceptional than the headline suggests, and not a result the county can replicate through its own decisions alone.
One of the concrete mechanisms behind this result deserves attention. In 2023, agency staffing (vuokratyö) accounted for 6 to 8% of the county's workforce in many service areas. By late 2025, that figure had dropped to roughly 1 to 2% of full-time equivalents [LUVN Palvelutuotannon kuukausikatsaus, December 2025; Uudenmaan Kokoomus review, March 2026]. In healthcare, agency staff can cost two to three times what permanent employees cost for the same hours. Rather than simply banning the practice and leaving gaps, the county built internal resource pools and focused on improving retention and working conditions for existing staff. The result is that what began as a short term cost saving measure is becoming a structural change in how the workforce is managed.
This fiscal outcome matters for two reasons. First, it buys the county breathing room. From 2027 onward, the fiscal environment is expected to ease somewhat, meaning the county can begin allocating resources toward service improvement rather than purely toward deficit recovery. Second, it validates the approach: structural cost reduction through service redesign, not indiscriminate cuts to frontline care.
The county's director, Sanna Svahn, has described the organisation as a "forerunner" in Finland's healthcare reform. At a time when the majority of Finland's 21 wellbeing services counties are struggling with deficits and many are unlikely to meet their balance targets, Western Uusimaa has crossed that threshold. Whether that makes it a forerunner or simply the least behind depends on what happens next.
What this means for the people who live here
I want to be careful not to turn a bureaucratic success story into something it is not. Hitting a surplus target does not mean the experience of care is where it needs to be. Waiting times remain a concern. Staffing pressures have not disappeared. The ongoing tension between county budgets and HUS cost demands is structural, and no single fiscal year will resolve it.
And the reform has produced real, measurable damage in places that rarely make it into strategy presentations. Before the county took over, doctors at municipal health centres in Espoo routinely referred patients to city-run sports and exercise services. In 2019, those referrals numbered over 300. By 2024, under the new county structure, they had collapsed to 58. The reason was simple: when health centres moved from city control to county control, the IT systems and referral pathways connecting doctors to municipal sports services broke. Nobody designed the new system to maintain that link. A preventive service that was working quietly and effectively was destroyed as collateral damage of an administrative transition. The county is now deploying a new system called LIIKUN to rebuild the connection, but the gap represents years of lost preventive care that did not need to happen [LUVN Services and Personnel Committee, December 2024].
It is also too early to know whether the county's flagship reforms are producing the outcomes they promise. Community living facilities are being built, but there is not yet meaningful data on whether they are reducing hospitalisations or improving quality of life for residents. The digital platform is being rolled out, but whether it is actually reducing unnecessary HUS referrals or just adding a new access layer on top of an unchanged system remains an open question. The strategies are sound. The evidence that they are working has not yet arrived.
But what the last three years have shown is that it is possible to build a functioning regional healthcare system from scratch, under extraordinary fiscal pressure, while simultaneously beginning to redesign how care is delivered. The community living strategy, the digital platform, the practitioner model at health centres, these are being implemented. Whether they are succeeding is a question for the next article.
For the roughly 500,000 residents of Western Uusimaa, including the 12% who speak Swedish as their first language and the growing number of residents who speak neither Finnish nor Swedish, the question going forward is whether this administrative machinery can translate its fiscal discipline into something they actually feel. The county holds a unique national mandate to develop Swedish-language health and social services for all of Finland, and the transformation of Raasepori Hospital into a bilingual centre of excellence is a central part of that mission. AI-assisted translation tools are being piloted, Swedish-language digital service pathways are under development, and the National Languages Board has pressed for bilingualism to be embedded into every shared pathway with HUS and partner municipalities [LUVN Budget 2025-2027; LUVN Services and Personnel Committee, December 2024]. For residents who speak neither official language, the stakes are even higher. These are the people for whom a well designed digital portal with multilingual capability could make the difference between accessing care and falling through the cracks entirely.
The foundation has been laid. The fiscal crisis has, for now, been navigated. The test from here is specific and measurable: do waiting times actually fall? Does the digital portal reduce hospital referrals or just add complexity? Do community living residents report better outcomes than those in institutional settings? Can a resident who speaks Somali or Arabic or Russian actually navigate this system without falling through the cracks? If the answer to those questions is still unclear two years from now, the surplus will have been a bookkeeping achievement, not a reform.
Sources
- Länsi-Uudenmaan hyvinvointialue. (2024). Talousarvio vuodelle 2025 ja taloussuunnitelma vuosille 2025-2027. Approved by Aluevaltuusto 10.12.2024. https://admin.luvn.fi/sites/default/files/2025-06/Länsi-Uudenmaan%20hyvinvointialueen%20talousarvio%20vuodelle%202025%20ja%20taloussuunnitelma%20vuosille%202025-2027.pdf
- Länsi-Uudenmaan hyvinvointialue. (2024). Press Release: Vuoden 2025 talousarvioesityksessä panostetaan palvelujen saatavuuteen. 23 October 2024. https://www.sttinfo.fi/tiedote/70609558/
- Länsi-Uudenmaan hyvinvointialue. (2025). Strategia. Updated strategy approved by Aluevaltuusto 7.10.2025. https://www.luvn.fi/lansi-uudenmaan-hyvinvointialueen-strategia
- Länsiväylä. (2026). Länsi-Uudenmaan hyvinvointialue ensimmäinen Suomessa, joka pystyi kattamaan aiempien vuosien alijäämät. April 2026. https://www.lansivayla.fi/paikalliset/9342011
- Länsi-Uusimaa. (2026). Länsi-Uudenmaan hyvinvointialue ensimmäinen Suomessa, joka pystyi kattamaan aiempien vuosien alijäämät. April 2026. https://www.lansi-uusimaa.fi/paikalliset/9342131
- Länsi-Uudenmaan hyvinvointialue. (2024). Palvelut ja henkilöstö -lautakunta, Pöytäkirja 16.12.2024. Services and Personnel Committee meeting minutes.
- Länsi-Uudenmaan hyvinvointialue. (2025). Palvelutuotannon kuukausikatsaus, December 2025. https://www.luvn.fi/fi/meilla-asiakkaana/palvelujen-saatavuus/palvelutuotannon-kuukausikatsaus
- Mäkäräinen, K. (2026). Mitä Länsi-Uudenmaan hyvinvointialueella tapahtui loppuvuodesta 2025? Uudenmaan Kokoomus, 23 March 2026. https://www.uudenmaankokoomus.fi/2026/03/23/mita-lansi-uudenmaan-hyvinvointialueella-tapahtui-loppuvuodesta-2025/